The ultimate comprehensive change
By Walter Sorochan Emeritus Professor San Diego State University
Posted January 12, updated October 11, 2021. Disclaimer The information presented here is for informative and educational purposes.
|
Abstract:This article is about fixing the current American health care system. It has implications for the entire world. The article addresses 8 key inter-related factors of health care. This information is targeted for main-street America so they can become more proactive and informed about health care. We need to view the health care system in all its complexity and not as a single dimension of cost control. Most of what makes up health care and causes high cost of health care is never discussed. The political debate about our health care crisis has been about bringing down the cost of health care and replacing the multi-payer system with a single payer universal heal care system. Both approaches have merit but are doomed to fail without making additional comprehensive 'must' paradigm changes. Even if we did adopt a universal single payer health care system, the adopted system would lower costs but would still be not work very well as there are many sub-parts[drivers] that are broken, not working very well and need to be fixed. The ideal way to fix a broken health care system would be to consider all eight inter-related factors that affect how health care is delivered to people --- the consumers. |
Fixing the broken health care system in United States is the unfinished business of the past 30 years. It will once again be revisited during election campaigns in 2020. Politicians and the public will rehash how to bring the high cost of health care system under control and ignore discussing better consumer quality care. Our health care system keeps on failing year after year. And each year our politicians fail to fix the health care system. The conversation since 2016 has been over reducing health care costs and not changing and improving the health care system itself. As of April 24, 2018, the issue of health care reform has been once again temporarily put on hold by more pressing presidential and world issues.
Meanwhile, the American public, frustrated with the dysfunctional political system and not understanding how the health care system should work, is left to survive on its own.
The debate over health care is not about health ... instead it has become about irresponsible and dysfunctional politicians. If we do not fix the political re-election financing system, then there is little hope of reducing health care costs and improving consumer wellbeing.
Health care is much more complicated than just bringing down the cost of health care or adopting universal health care. Most of what MAKES UP health care is never discussed. It is taboo! That is what this article is about .... what is never discussed.
Many persons have an opinion about what is wrong with our health care system [1] Jaffe: What's wrong US health care? 2016 [2] Kliff What is wrong with health care 2014 [3] Gilchrist: Cuban fixing hea care 2017 [4] Hahn: Fixing health care system 2016 [5] Hugin: How fis system 2018 [6] Morrison: Fix hea care sys 2017 [7] Sachs: Saving money 2017 [8] Varsavsky: Fix hea care sys 2018 [80] Consumer Reports: Hazardous coverage 2009
|
Author Background Walter Sorochan has a a very good background in health, medicine and public health. He taught numerous courses at the university, including personal health, environmental and international health. He was fortunate to be exposed to Dr.Charlie Ross, MD., and his health promotion programs in Indianapolis and San Diego. for several years during the early 1980s. In 1996, he worked with a family physician in San Diego to streamline the paper records in his medical office with an electronic patient record system [now referred to as Electronic Health Records]. This included interfacing electronically many state and local services .... a task far ahead of its time. We ran out on money even though the data entry and all other features were 90% complete and functioning. Needless to say, this was a great learning experience. Finally, as a patient and subscriber, I learned a lot just being part of the Kaiser Permanente health care system for over 45 years. I had an opportunity to observe how hospitals and doctors work after several surgeries, ER visits and regular visits for medical checkups. |
Well, here is one health consumer, after much thought and experience in the health care system, who would like to voice his opinion about how to not just fix a broken health care system, but also bring the cost down and improve the wellbeing for everyone.
So what is broken in the health care system today?
We need to view the health care system in all its complexity and not as a single dimension of cot control. This article addresses 8 key inter-related factors of health care.
Consumers view a broken health care system that does not serve them while politicians view the high cost of health care. Politicians contend that as people get older, they are being treated for many chronic diseases; and that such treatments cost so much money that the present health care system is unsustainable. Politicians blame people, as consumers, as the reason health care is so expensive. But this contention is not the whole truth, for the current health care system design itself has been causing most of the high cost and has been failing for a long time.
Caregivers have their view of what is broken in the health care system while politicians view the high cost of health care. Politicians contend that as people get older, they are being treated for many chronic diseases; and that such treatments cost so much money that the present health care system is unsustainable. Politicians blame people, as consumers, as the reason health care is so expensive. But this contention is not the whole truth, for the health care system paradigm itself has been causing most of the high cost and has been failing for a long time.
Politicians argue about runaway health care costs but fail to identify and fix the real causes of a broken health care system. One cannot fix something when one ignores reality or does not know what caused it to be broken. Likewise with health care .... you need to know what parts of the system are broken and not working. This article focuses on eight major factors that would ideally fix our health care system.
Today, health economists are alarmed about the uncontrolled costs of chronic diseases. [10] Fried: need to prevent chronic diseases 2017 [11] Huffman: Chronic diseases - today & tomorrow [ 12] Padula: Preventing chronic diseases 2012 Chronic diseases account for 86% of our nation’s health care costs and many chronic diseases are on the rise. [13] Bauer: failings of modern medicine 2014 [14] Horowitz: Fixing our health care System 2017 [15] McGreal: Opioid epidemic 2017 It is also true that most of the 7 out of 10 deaths due to chronic health conditions are largely preventable. [16] Flottemesch Savings from prevention 2010 [17] Christensen: health for hire 2017
There is also ample evidence that the high cost of chronic diseases can be lowered by prevention. [18] Getlen: US broken health care system 2017 [19] Psaltopoulou: Psaltopoulou: dif-lifestyle & prevention 2010 80% of cardiovascular diseases and 60% of all cancers could be prevented, but not with the existing health care system we have today. [21] Sorochan: Whole Body Wellness 2017
The flaw in thinking about fixing our health care system?
Numerous persons [22] Angell: Drug-doctor corruption 2009 [23] Feld: Repairing the healthcare system [24] Fried: need to prevent chronic diseases 2017 [25] Gross: US Health care big business 2017 [26] Padula: Preventing chronic diseases 2012 [28] Mahary: Why system broken 2015 including presidential candidates, have suggested fixing our broken health care system by implementing universal health care. But such fixes may not be comprehensive, and do not fix all the inner broken or dysfunctional parts of the system. It is wishful thinking that if we change to a single payer system, then our health problems will be solved; yes, the cost would be lowered but not improve the delivery of health care nor improve the quality of consumer care.
This is where much of the political state of mind is today. But we cannot just revert to a single payer universal health care system, for the "hidden system" issues that cause chronic diseases would still be there [ like wide range of interactions, fee schedules for drugs and supplies, strategic/unsavory billing, practice coding, rationed price negotiations, AMA super PACs raising lobbying/election money. [29] Rosenthal: An American Sickness 2017
 History
of health care in USA: It may be helpful for the reader to understand how United States got into this health care
system mess by briefly reviewing the history of how the current health care
system evolved:
History
of health care in USA: It may be helpful for the reader to understand how United States got into this health care
system mess by briefly reviewing the history of how the current health care
system evolved:
The practice of Western medicine today stems from belief in the germ theory and the Flexner Report published in 1910.
The practice of Western medicine today stems from belief in the germ theory and the Flexner Report published in 1910. Below is a brief summary of the disease paradigm, how, since 1800, doctors have tried to explain the meaning of health and medicine. For example, two systems of medicine, one based on Pasteur's germ theory [ monomorphism ] and the other on Bechamp’s cellular theory [ pleomorphism ].
Below is a brief summary of the disease paradigm, how, since 1800, doctors have tried to explain the meaning of health and medicine. For example, two systems of medicine, one based on Pasteur's germ theory [ monomorphism ] and the other on Bechamp’s cellular theory [ pleomorphism ].
Much of the origin of the medical belief system originated with Pasteur's germ theory of monomorphism. That is, most disease is caused by germs or some form of static, disease-causing microbe outside the body [the germ theory]. In order to get well, you should KILL the germs .... and that is where drugs and antibiotics come into use. The other theory of medicine, Bechamp's Cellular Theory, states that diseases arise from micro-organisms within the body. Sorochan: New medical Revolution 2012
|
The Disease Paradigm Pasteur's Germ Theory: "One school of thought (modern medicine and the monomorphic perspective) says most disease is caused by germs or some form of static, disease-causing microbe (the germ theory) from outside the body. In order to get well, you should KILL the germs. KILL the microbes. KILL whatever is making you sick. Drugs, antibiotics, chemotherapy, radiation, surgery. Bechamp's Cellular Theory: The other school of thought (which encompasses most other forms of the healing arts unrelated to mainstream medicine) says most disease is caused by some unbalance in the body. The unbalance occurs in some nutritional, electrical, structural, toxicological or biological equation. In order to get well, you need to re-establish balance in your body by working with your body, not against it." [81] Cowan: Pleomorphism |
Since that early era, many astute scientists and doctors [ Enderlein, Rife, Reich, Livingston-Wheeler, Naessens, over the past 100 years have challenged the monomorphism theory and the medical practice of today. [83] Donohoe: New Medical Theory 2007
The second impact on the health care system and medical practice was the Flexner Report. The current American health care system was designed to provide better health care at the beginning of 1910, when the Flexner Report [30] Wikipedia Flexner Report [86] Flexner: Med Education Report 1910 laid out standardizing medical training and improving medical practice. During this early time, improved sanitation and a better diet had already started a trend for better health in the general population. Communicable diseases were being brought under control.
As a reminder, health care, lifestyles and eating habits in 1910 were totally different from those of today. While many medical doctors began private practice from 1910 through 1950, their patients had difficulty paying for services. Most persons were not insured for possible health disasters.
Although many persons suffered from cancer, heart disease and other chronic diseases, most persons in the 1920 -1940 era had better food choices than we do now, and probably enjoyed better health than many do today. Many people during this early era self healed and many seldom went to doctors because they could not afford doctor care.
After world war II, there was a resurgence to further improve health care. Hospitals, with little control, were built that eventually offered expensive therapies allowing doctors to use these therapies to treat their patients. Penicillin and antibiotics helped control infections.
Health insurance began evolving after the end of WWII. Insurance companies originally began to offer insurance for time lost from work; later offered insurance that dealt with short term injuries and catastrophic illnesses and then began offering more comprehensive coverage for hospitals, drugs and doctors. Doctors practicing specialty medicine requiring expensive diagnostic tools were covered by insurances.
It was about 1970 when our lifestyles and food choices began changing with food stores offering processed foods using additive sugar, fat and salt. Fast foods and restaurants began displacing home cooking. These were significant lifestyle changes that began changing how we lived, what we ate and how our bodies responded. Lifestyles slowly and silently began changing short term illnesses into chronic diseases. Seniors living beyond 80 years of age, approaching end of life time, were gradually impacting on health insurance and end of life medical expenses.
The widespread acceptance of health insurance coverage gave birth to how hospitals, doctors and drug companies chased money. It made health care a super expensive industry that was tied to government reimbursements. About 1980, the good intentions of the Flexner health care system of continually improving the health of people were hi-jacked by the medical-industrial complex [service providers like drug, insurance, hospitals and medical supply companies and doctors]. It was this trend of emerging changes that caused the current health care system to become expensive, inefficient, and that overlooked serving good care to people.
Incidentally, the Flexner Report made recommendations, based on the germ theory, to improve the quality of medical education, and how medicine was to be practiced. Flexner did not define health nor health care. The medical belief system has changed very little since then. Yes, we have had some wonderful advancements in public health, surgery and drug therapy. Despite all the self praise of the medical establishment, little progress has been made to bring chronic degenerative diseases like cancer and heart disease under control.
Over time, the delivery of care has been designed around doctors, providers and institutions, but not around the patient or consumers. [85] Steinreich: !00 years of medicine 2010
Fast track to today. Politicians in 2017 - 2019 have focused on reducing health care costs instead of revamping the dysfunctional and outdated the health care system itself. A diversion from reality!
So, how do we fix a broken system?
There has been considerable debate and much misinformation, since 2000, about replacing the multi-insurance system with a single universal health care system. The hope was that implementing a universal health care system would provide an instant comprehensive working model that would solve many of the systemic problems. But this did not happen!
The argument of lowering the cost of the single health care deliver system overshadows all the other factors that impact on provider delivery and consumer quality care. Politicians neglect to talk about these other factors This is what we neglect to talk about and this matters, for it keeps consumers uninformed and passive.
What should a good working health care system include? The logical place to start would be with an ideal paradigm. Below is a circle displaying eight factors that need to be considered in such a revised and ideal paradigm:
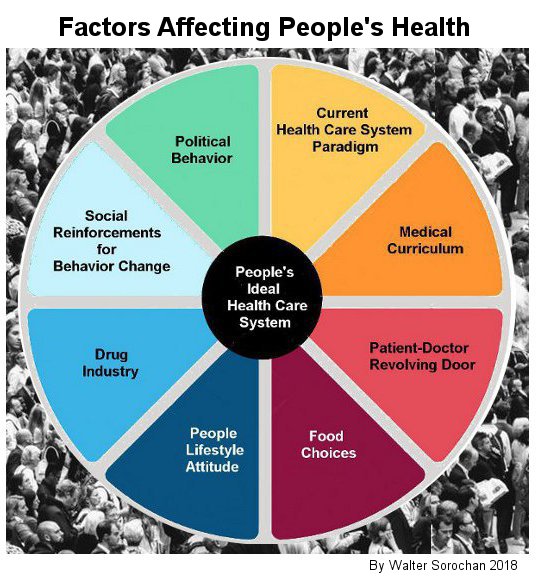
Politicians in the past have swept seven of these factors under the carpet and avoid discussing them.
Although most health experts agree that chronic diseases are caused by self-destructive lifestyles, medical doctors Ezekiel and Rosenthal and others [35] Fried: need to prevent chronic diseases 2017 [36] Gross: US Health care big business 2017 [37] Huffman: Chronic diseases - today & tomorrow [38] Jaffe: What's wrong with US health care? 2016 [40] Mattke: Rand-Home health care 2010 [41] Padula: Preventing chronic diseases 2012 [42] Shaw: Chronic disease theories 2017 [43] Weiss: Medical rip-off , point out that the medical system itself has a vested reason to perpetuate the drug treatment model and ignore identifying the cause(s) of chronic diseases. [44] Shackelford: MD shocked at cost & service 2015 In other words, keep the current health care system as it is because it is a cash cow for providers.
Providing comprehensive health care for people is more than just fixing a broken health care system. It must include all the 9 inter-related factors impacting on the delivery of comprehensive health to all people:
1. Current health care system paradigm is a huge part of the big problem of health care. There are may things we can do to lower the cost of health care and provider quality care to everyone. The list is not all inclusive:
Insurance fear misinformation argument: Proponents of today's multi-insurance health care system advance the "fear argument" that universal health care is socialized medicine and so we need to keep the current multi-health insurance entities system. We can dispel such fear misinformation by understanding how the universal health care works. Many people who believe they have adequate health insurance actually have coverage so riddled with loopholes, limits, exclusions, and gotchas that it won't come close to covering their expenses if they fall seriously ill. Read: [84] Consumer Reports: Hazardous coverage 2009
Much of the misinformation comes from politicians and most Americans are not aware or do not understand how insurance works.
How insurance works: The most important aspect of universal health care, that makes it work, is "numbers" concept. Two numbers are important here. Most persons are faced with the premim cost of health insurance and this is the first number. How much you will pay for health care insurance is the first number thrown at people by insurance companies. The second number is hidden, not discussed and not seen by consumers .... is the size of the insurance company, or the number of people in the insurance package. This is the most important number. It tells us which insurance companies are big and which are small. The larger the pool of people covered in the second numbers package, the less cost of the premium insurance. It is this concept of large numbers of people that makes the insurance premium of each insured person cost less. It is this hidden number of person subscribers in the membership pool that tells you what the cost of your health insurance policy will cost. Although this membership pool number should imply the cost of a policy, it still does not account for the small print disclosures of what is covered and not covered in the [secret] policy, the deductibles and how much per month you would pay.
Universal health care is based on LARGE numbers. That is, the more persons in the population insurance pot, the lower the cost of health insurance. [45] Rosenthal: Costs of health care [46] Sorochan: How insurance works 2014 On the other hand, most private insurance companies need to charge high premiums because their smaller people base is a higher cost payout risk and has to cover catastrophic incidents that are spread over a smaller membership pool.
Lower cost in a universal health care system allows most persons to be able to afford health care insurance. [47] Sorochan: How insurance works 2014
There is also a misconception that multi-insurance health care system would prevent chronic diseases and prevent its spiraling costs. [48] Brodwin: Advanced countries view US Health care 2017 Yes, the big insured population number would dramatically reduce health care costs. But health care system models are full of imperfections and, as already pointed out, these need to be fixed in order to provide better health care and further bring the cost down. Fro example, the current health care system and medical practice is based on prescribing dur medications for pain instead offinding and fixing the real cause of pain. Instead, the medical care system needs to change to a preventive model.
Lack of affordability: "Even after implementation of the Affordable Health Care Act, millions of Americans still remain uninsured. The current health care system is not affordable to the majority of Americans. Many simply cannot afford the cost of today's health care insurance. More often than not, the health coverage they get is not comprehensive and is limited in scope.
United States is the only country in the world that does not have a single-payer universal health care system. If we had Canada’s single payer national health care system, we could save no less than $13,600 per average household. That adds up to a walloping $1.7 trillion dollars for the U.S.. [51] Komlos: KPBS What's wrong with US hea care sys 2017
The Canadian example of reduced health care costs is a big plus. But there would be other savings if we were to fine tune the universal health care system. 20% or more of total health care expenditures, such as various forms of waste, including overtreatment, failures of care coordination, failures of care delivery, administrative complexity, pricing failures and fraud and abuse, if eliminated, could be additional savings. [52] Kaiser Report 2012
Unnecessary spending in the US health care system: There are compelling signals that much of health spending does little to improve health, and, in certain circumstances, may be associated with poorer health outcomes. [58] Yong: Lowering medical costs 2010
"Some have estimated that 20% or more of total health care expenditures is due to various forms of waste, including overtreatment, failures of care coordination, failures of care delivery, administrative complexity, pricing failures and fraud and abuse. Waste is exemplified by unnecessary or inappropriate treatments and tests, inefficiencies in medical care delivery and financing, encouraging the use of specialists or profitable equipment, and the lack of integrated, efficient systems to electronically store and transmit health data. [59] Kaiser Report 2012
Lack of comprehensive coverage: A major flaw in health care coverage is that it is often not comprehensive. There are many health issues today that fall through the cracks. Just three examples illustrate how comprehensive health coverage has fallen through the cracks affecting all ages:
• Dental health coverage is excluded from the health care system in United States. Although comprehensive dental insurance coverage is available separately, it is expensive, rationed and most persons cannot afford good coverage. Most dental programs cover cleaning teeth but then charge thousands of dollars out of pocket for fixing other dental problems. More often than not, fixing teeth is postponed.
• Mental illnesses have been largely ignored since mental hospitals were abandoned in the mid 1960s. Many mentally ill persons are dumped on the street and become homeless persons. Many of these street people are war veterans coming home suffering emotional trauma from killing real people and difficulties in being re-absorbed back into society. Others suffer with brain concussion [shell shock] injuries from being exposed to bomb explosions. These brain concussion injuries are very similar to those experienced by football athletes. Help for mentally sick persons and especially returning war veterans has been basically overlooked in United States. You cannot sugar coat brain injured veterans with lip service and money.
• Education: We would also save a ton of money in the long run if we educated school children and teen agers how to prevent chronic diseases early and have them continue prevention throughout life, before they become old. [53] Mattke: Home health care 2010 Yes, we would still need to pay for the older persons end of life expenses, but the expenses would be much reduced.
Providers under one umbrella: Another way of reducing the cost of health care is to bring the different divisions of health care in government under one umbrella. Different divisions or segments of the health care system are duplicated, tend to protect their turf and do not communicate with each other very well. Such mis-communications increase the cost of health care.
Components of health care are scattered throughout the federal and state systems. For example, Centers for Disease Control & Prevention [CDC], National Institutes of Health [NIH], Centers for Medicare and Medicaid Services, Department of Agriculture, Department of Environmental Protection [EPA], Veteran's Health Care and Health and Human Services .... each vie for a piece of the health pie. We need the health care system to be under one umbrella so the right hand agrees with what the left hand is doing! [54] US Health Agencies [55] Brodwin: Advanced countries view US Health care 2017
Free market: Another issue related to the universal health care system is the assumption that the health care system is a free market. Many have been misinformed that health-medical care can be priced the same way as consumer and industrial products. As a country we tend to cling to the misguided belief that all markets are the same, always and everywhere necessarily efficient and that competition regulates cost. This is patently false, however, as the Nobel Prize-winning economist Joseph Stiglitz has pointed out.: "In the case of the medical system, clinging to an outdated ideology is nothing less than a disaster. Why? Because the medical industry is unique, and we’ve known this for a very long time. "As the economist Kenneth Arrow, another Nobel Prize winner, argued as far back as 1963, free markets in health care are inefficient because of the “existence of uncertainty in the incidence of disease and in the efficacy of treatment.” [56] Komlos: KPBS What's wrong with US hea care sys 2017 We need transparency price competition in a free market.
Lack standardized pricing: Health care costs lack standard pricing for the same surgery or service and vary from state to state and city to city. Medical doctor turned medical reporter, Elizabeth Rosenthal, cites an example of a echocardiogram lab test that costs $1000 at one of the nation's leading academic hospitals, then costs $ 7000 at a small community hospital in New Jersey --- and the equivalent of only $100 in Germany and Japan. [57] Rosenthal: Costs of health care We have a poorly regulated medical market.
Many doctors support changing the medical practice of today to a functional paradigm. [31] Feld: Repairing the healthcare system [32] Rosenthal: Costs of health care [33] Rosenthal: An American Sickness 2017 [34] Emanuel: Future health care system 2017
Adopting Universal Health Care: It is time for Americans to adopt a single-payer system, also referred to as universal health care, like the ones in other developed capitalist countries like Canada, Sweden, Germany and Australia. The universal health care systems in these and other countries work better than in United States by bringing down the cost of health care. But these systems in other countries may not be working as well as they should, for these foreign single-payer health care systems also have many aspects of the wrong health care paradigm.
These are just a few shortcomings of our current health care system that would reduce cost and provide better health care.
2. Medical curriculum in medical schools must to be upgraded to serve the people and not perpetuate medical practice as a convenience for doctors and the medical-industrial complex. We need a new paradigm for the practice of medicine. Medicine needs to revamp how doctors practice health care and also change the medical curriculum in medical schools. [62] Horowitz: Fixing our health care System 2017
Medical doctors Farshad Fani Marvasti and Randall S. Stafford [60] Marvasti: re-engineering health care 2012 argue that medical schools need to change their curriculum: "to combat the primacy of technical knowledge and the profit-based system for medical technology, medical schools must teach prevention strategies alongside treatment approaches and emphasize motivational interviewing with a focus on lifestyle modification. Payers and the federal government must fully reward use of appropriate non-patentable therapies and support research on the development and dissemination of prevention strategies." [61] Marvasti: re-engineering health care 2012
A major issue that needs to be resolved in the medical paradigm is the conflict between Pasteur’s germ theory [ monomorphism ] and Bechamp’s cellular theory [ pleomorphism ]. This is already an issue that is happening with orthodox or conventional vs. unconventional medicine today. The contributions of both medical theories and models need to be recognized and molded into a working model of comprehensive health care. For more information on this issue, refer to: [62] Sorochan: New medical Revolution 2012
Today, the medical curriculum reflects the interests of health care providers which is not the same as the needs of consumers. Providers deliver a response to symptoms of a sick person but seldom deal directly with the causes of a disorder or disease. Medical schools prepare prospective doctors to accept the current health care system. We have a medical symptoms treatment for profit model and not a disease prevention and wellness model. This reflects a huge difference between provider medicine and consumer health!
Medicine must change from treating symptoms of pain and discomfort [where the real money is] to also finding the cause of pain, inflammation and discomfort and preventing disorders and diseases [ where healing and health is].
Our outdated healthcare system has been designed primarily for acute emergency illness and injury and not for long lasting chronic diseases nor taking care of an aging population. The present model [paradigm] for treating acute infectious disease is being misapplied to the treatment of chronic disease; consequently the current health care system has the wrong paradigm design. Today's multi-payer health care system avoids focusing on the real cause of chronic diseases .... people eating wrong food. Instead it focuses on drug therapy creating a culture that appears to devalue disease prevention. [63] Rosenthal: An American Sickness 2017
Medical doctors need to go to school to learn about nutrition and validate their outdated medical licenses as medical knowledge is doubling every six to eight years. [64] Moynihan: Health future is now 2016
Medical schools need to include nutrition and food in their curriculum. Most doctors today seldom if ever ask their patients what they eat. They never do a diet analysis of what their patients eat for a week. Why is it that most doctors avoid talking about food and nutrition with their patients? The answer is provided by an AMA staffer [65] AMA: Nutrition status in medical schools 2015 reporting that only 27 percent of U.S. medical schools actually offer students the recommended 25 hours of nutritional training. Practicing physicians continually rate their nutrition knowledge and skills as inadequate. [66] Adams: Nurtition education in medical schools 2011
Lifestyle [orthobiosis] itself is a tricky issue, especially if the doctor has not had any nutrition classes in medical school, is uninformed about nutrition, and has been indoctrinated that drugs heal and food is what you eat when you are hungry. The major part of lifestyle change is food and nutrition; not drug prescription.
The curriculum in medical schools also needs to change the medical-disease belief system and focus on multiple diseases. Patients may be harboring two or more health problems that vacillate and incubate at the same time on a long term basis; that doctors need to treat at the same time. Such ticking time-bomb diseases are not being tracked in an effective manner.
Marvesti points out that "the original approach to medicine endorsed by the Flexner report succeeded because it was based on sound science and a radical restructuring of the way medicine was taught, organized, and practiced. Today, we face a similar challenge that requires another fundamental reordering of our health care system. Although the need for acute care will remain, centering our efforts on prevention is the only way to thwart the emerging pandemic of chronic disease." [67] Marvasti: re-engineering health care 2012
Fixing the current medical paradigm, that is, the many "inner" aspects of medical school curriculae, would bring change to medical practice. These are the recommendations of astute and experienced medical doctors.
3. Patient-doctor revolving door: prescriptions are another part of the major fix equation.
The medical practice of people running to their doctor all the time needs to change. People have been brain trained to run to their doctor or ER when sick or for whatever ails them. Many of their health problems are treated for symptoms of pain, inflammation and discomfort. When the prescription runs out and the pain comes back, the sick person once again runs to the doctor to renew the pills. This is business as usual!
This 'medical-symptoms-prescription revolving door' procedure lures the person-patient to outsource their body and health to the care of the doctor. In doing so, the person gives up most responsibility for taking care of her/his health. This is a major practice that needs to be reversed. The patient needs to take back her/his body, update personal hygiene, learn how to prevent getting sick, learn to self-heal, learn nutrition and make good food choices; while keeping the doctor as a backup. This would go a long way in reducing costs and the need for more medical doctors.
4. Food choices: The major lifestyle change is the food we eat. [68] Psaltopoulou: Psaltopoulou: dif-lifestyle & prevention 2010 [69] Coulston: Disease prevention/treatment Most medical doctors do not perceive food as a medicine and disease preventative. Food is another needed medical curriculum change.
Eating is complicated and very few really understand it. There are good and bad foods. A big problem with food is that most persons eat processed foods. Many processed foods have many nutrients removed and instead, have addicting chemicals added to them, like sugar, salt and fat, to make food taste better and last longer on the grocery shelf. Human bodies are very sensitive, complex and precise machines that can instantly recognize bad foods and try to store fat. So to change food habits, people need to change their addictions. Instead of habit-addicting foods, people need to learn to make wiser food choices.
Incidentally, bad foods feed the bad bacteria in one's colon that, in turn, cause many chronic diseases [side effects]. On the other hand, good healthy foods feed good bacteria that enhance immunity, prevent diseases and enhance wellbeing. It should be obvious to everyone, and especially medical doctors and politicians, that food is a medicine that heals and prevents.
5. People's lifestyle attitude: to change how they live. The real big fix is changing the lifestyles of people, helping them make wiser food choices, assuming more self responsibility for healing, exercising more often, preventing chronic diseases starting at an early age and using the health care system more effectively.
People need to re-learn how to prevent illnesses and diseases, begin assuming more self-help-self-care by taking first aid emergency-preventive classes [not standard Red Cross classes], learn about good and bad foods and how these can affect their wellbeing; and use doctors as a backup when needed, like essential surgery. This transition of having people assume greater responsibility for maintaining their health is just as important as making health care system changes. [70] Christensen: health for hire 2017 Such transitioning needs to start in early childhood and continued into older age. Doing so would result in fewer visits to doctors and ERs and lower the cost of health care.
To prevent and reduce the cost of managing chronic disease, "the system must learn to facilitate change in individual behavior, which has the greatest impact on health status of any contributing factor, including healthcare." [71] Christensen: health for hire 2017
6. Drug industry is out of control: The current medical curriculum is sponsored by Big Pharma. Drug companies have become the most profitable and powerful, unregulated, major industry in the country. "Price gouging in the US pharmaceutical drug industry goes back more than three decades. [72] Lazonick: Pharma business model 2017
Lynn Parramore, the Senior Research Analyst for the Institute for New Economic Thinking [74] Parramore: Pharma fuels opioids 2017 , points out that Pharma influences the government in setting drug prices, manipulates prescription drug prices, dictates drug policy to the federal government and impacts on university research and programs. High drug prices restrict access to medicines and undermine medical innovation. Lax drug regulations mislead doctors and patients about the safety of drugs. Much of the R&D work on new drugs is taxpayer-funded at universities and then usurped by Pharma. Many experts agree that US drug industries have become monopolies and need to be regulated:
Marcia Angell observed in her last editorial in the NEJM, "drug corporate influence in medicine is ubiquitous, extending far beyond individual physician-researchers: its influence determines what research is conducted, how it is done, and the way it is reported. Drug corporations endow academic chairs and programs, impact the medical curriculum, provide grants, stock equity, and often pay patent royalty fees to researchers and institutions." [75] Hassner: Conflicts of interest 2002
Drug conflicts of interest affect more than research. They also directly shape the way medicine is practiced, through their influence on practice guidelines issued by professional and governmental bodies, and through their effects on FDA decisions. [76] Angell: Drug-doctor corruption 2009
The drug companies silently impact all aspects of our lives.
7. National & Social reinforcements: Another big, hidden and unspoken needed change is national and social reinforcements to support positive lifestyle changes. It is difficult to change bad food habits when TV advertisements and commercial adds portray affluence by displaying junk food, sugar drinks and drug cures for everything: "Take a pill and munch junk food while you watch TV". Many countries, other than United States, outlaw TV commercials advocating junk food and drugs! We need social and economic reinforcements on a continual basis to remind everyone to eat good foods and enhance optimal wellbeing.
8. Changing how politics work: is a must: None of the other fixes will work if politics is not changed! Our politicians are bought with election money by big Pharma, hospitals and insurance companies to do their bidding at the expense of ignoring the real needs of people. An example of this is America’s opioid crisis that was caused by parana Pharma companies, politicians who colluded with them and political regulators who approved one opioid pill after another. [77] McGreal: Opioid epidemic 2017 The opioid crisis is itself an urgency for the medical-industrial complex to change.
9. Understanding how the human body works: It is this author's belief, from reviewing hundreds of articles about health, health care and medical practice, that most medical doctors prescribe therapy but seldom find time to elaborate on how the human body works. Furthermore, most persons do not understand how their body works! It is this lack of 'how the body works' that can be the change agent in prevention and behavior change. Using a fear tactic by telling the obese patient to lose 'weight or else' carries little motivation to do so. The overweight/obese person needs to know how the body works in a healthy, non-obese body and how obesity incubates other chronic diseases. Knowledge is an ignored weapon!
Conclusion: It is time to become honest, realistic and face the truth. Eight supporting factors are essential and need to be coordinated for all of us to enjoy good health and be more economically productive. Although these are the most relevant 9 factors that are linked to our health care system, the underlying factor is public education and especially health preventive education of the young.
Preventive health education is missing in our public schools today. Yes, a few schools may have drug and sex education but this is not comprehensive health education that is needed to help youngsters understand how to prevent infections and diseases and practice preventive health care on a continuous basis. Parents and the older population likewise lack understanding how to deal with diseases and wellbeing. Public health education could easily have been included as the 9th factor.
It is well known that most persons do not know very much about health care; that is, about the health care system, about their own personal wellbeing and especially disease prevention. It is with this awareness that this article was evolved. The information herein, though limited in detail and scope, is intended to make the general public more aware and informed of what we need to do to get better, save money and prevent chronic diseases.
Ofcourse these 9 factors are sensitive issues. Obviously we cannot change all of these at the same time .... but this is not a good excuse not to try and start with a few changes. With the 2020 mid-election coming up in November, 2020, fixing the health care system will be a hot candidate issue once again. It will not go away!
Politicians need to finish fixing the outdated health care system. The nine causes, that have been identified as essential consideration to fixing the health care system, may be overwhelming and scary but these are very real considerations. You cannot fix just one or two aspects of a broken system and expect the rest of the system to fall into place .... and lower costs and provide better health. These eight are like the pieces of a jigsaw puzzle. You need all nine to fit together in order to see the picture and the puzzle to work. And so it is with fixing the entire health care system for consumers.
There are also many minor inner problems that are not mentioned that would also need to be changed. Health care experts can draft a priority list on where to start, making changes to the current health care system paradigm. The most essential need for change is how we do politics. Unless we fix the political system, we will never be able to fix the health care system. A second good place to start would be getting medical doctors to become a unifying force for change, adopting universal health care; then making changes in the medical school curriculum and public education. We need to implement the essentials of food, nutrition and disease prevention into medical education and the school health curriculum. Everyone needs to assume more responsibility for self-care.
The real fix needs to be how we do politics. Unless we fix the political system, we will never be able to fix the health care system. Another good place to start would be getting medical doctors to become a unifying force for change, adopting universal health care; then making changes in the medical school curriculum and public education. We need to implement the essentials of food, nutrition and disease prevention into the school health curriculum. Everyone needs to assume more responsibility for self-care.
All the bad things about our health care system and how we live can be changed. "Study after study shows that primary and preventive care greatly reduces future health care costs, as well as improving patients' health.” [78] Cohen: Prevention & politics 20108 "Switching the focus from treating to preventing the chronic illnesses will not only improve the health of individuals, families and communities all over the country, but will also rein in health care costs and strengthen the economy!" [79] Padula: Preventingchronic diseases 2012,
Jeffrey Sachs, university professor and director of the Center for Sustainable Development at Columbia University, has focused very aptly: “None of this is rocket science. Nor is the United States too dumb to figure out what Canada, the UK, France, the Netherlands, Germany, Japan, Sweden, Norway, Denmark, Finland, Austria, Belgium, Korea and others have solved. The problem is not our intelligence. The problem is our corrupt political system, which caters to the health care lobby, not to the needs of the people.” [85]
Change is slow and hard to come by. While we wait for politicians to pass legislation and do the right thing, we should become proactive and take steps on our own to prevent diseases.
References:
[1] Jaffe Richard, "What's wrong with American health care?" Richard Jaffee Esq Lawyer, April 2, 2016. Jaffe: What's wrong US health care? 2016. Jaffe: What's wrong with US health care? 2016
[2] Kliff Sarah, "8 facts that explain what’s wrong with American health care," Physicians for a National Health program, September 2, 2014. Article by Kliff What is wrong with health care2014 no longer active.
[3] Gilchrist Karen, "Mark Cuban sees a model for fixing health care — and he didn’t find it in the United States," CNBC News, July 31, 2017. Gilchrist: Cuban fixing hea care 2017 Gilchrist: Cuban fixing hea care 2017
[4] Hahn Mathew, "Fixing the American health care system is simple. Here’s how to do it," MedPage, October 25, 2017. Hahn: Fixing health care system 2016
[5] Hugin Robert J., "How we can fix our broken health-care system," CNBC News, February 13, 2018. Hugin: How fix system 2018
[6] Morrison Pat, "The US medical system is broken. We should be listening to doctors about how to fix it." Los Angles Times, July 05, 2017. Morrison: Fix hea care sys 2017
[7] Sachs Jeffery, "America can save $1 trillion and get better health care," CNN News, June 27, 2017. Sachs: Saving money 2017
[8] Varsavsky, Martin, "How to fix US health care," Huffington Post, January 07, 2018. Varsavsky: Fix hea care sys 2018
[9] Yong Pierre L., Robert S. Saunders, and LeighAnne Olsen, THE HEALTHCARE IMPERATIVE Lowering Costs and Improving Outcomes, Institute of Medicine, The National Academies press, 2010. Yong: Lowering medical costs 2010
[10] Fried Linda P., "America’s Health And Health Care Depend On Preventing Chronic Disease," Huffington Post, March 14, 2017. Fried: need to prevent chronic diseases 2017
[11] Huffman David, "Chronic Disease Today and Tomorrow," Powerpoint presentation. Huffman: Chronic diseases - today & tomorrow
[12] Padula Caitlin, "The affordable care act: Preventing chronic diseases, The Blog, April 09, 2012. Padula: Preventing chronic diseases 2012
[13] Bauer Henry, "The failings of modern medicine," Explorer, November/December, 2014. Vol 10, No. 6, 345. Bauer: failings of modern medicine 2014
[14] Horowitz Richard, "Want to Fix Our Health Care System?" Huffington Post, March 08, 2017. Horowitz: Fixing our health care System 2017
[15] McGreal Chris, "Don't blame addicts for America's opioid crisis. Here are the real culprits," The Guardian, August 13, 2017. McGreal: Opioid epidemic 2017
[16] Flottemesch Thomas J., Michael V. Maciosek, Nichol M. Edwards, and Leif I. Solberg, Health Partners Research Foundation and Ashley B. Coffield, "Cost savings from primary and secondary prevention," in Book summary by Yong Pierre L. and others, 2010. Flottemesch Savings from prevention 2010
[17] Christensen Clayton, Rebecca Fogg and Andrew Waldeck, "Health for hire: Unleasing patient potential to reduce chronic disease costs," Christensen Institute Innosight, October, 2017. Christensen: health for hire 2017
[18] Getlen Larry, "5 scary facts about America’s broken health care system," New York Post, May 6, 2017. [Time to Address Emerging Infections and Environmental Toxins: Let the CDC and EPA Do Their Job!]. Getlen: US broken health care system 2017
[19] Pearl Robert, Mistreated [book summary], Public Affairs, Mew York, 2017. 2017. Article by Pearl: Mistreated 2017 is inactive.
[20] Psaltopoulou Theodora, Ioannis Ilias, and Maria Alevizaki, "The Role of Diet and Lifestyle in Primary, Secondary, and Tertiary Diabetes Prevention: A Review of Meta-Analyses," Rev Diabet Stud. 2010, May 10; 7(1): 26–35. Psaltopoulou: dif-lifestyle & prevention 2010. Psaltopoulou: Psaltopoulou: dif-lifestyle & prevention 2010
[21] Sorochan Walter, Whole Body Wellness 2017 [Paperback] Sorochan: Whole Body Wellness 2017. Sorochan: Whole Body Wellness 2017
[22] Angell Marcia, ""Drug Companies & Doctors: A Story of Corruption," Honest Medicine, New York Review of Books, January 15, 2009. Angell: Drug-doctor corruption 2009
[23] Feld Stanley, "Repairing the Healthcare System," Feld: Repairing the healthcare system
[24] Fried, ibid. Fried: need to prevent chronic diseases 2017
[25] Gross Terry, "How U.S. Health Care Became Big Business," HEALTH INC., April 10, 2017. [Author of book: An American Sickness] Gross: US Health care big business 2017
[26] Padula, ibid. Padula: Preventing chronic diseases 2012
[27] Pearl, ibid. Pearl: Mistreated 2017
[28] Makary Marty,"Why our health care system is broken," CNN, December 28, 2015. Mahary: Why system broken 2015
[29] Rosenthal Elizabeth, An American Sickness: How Healthcare Became Big Business, Amazon, [book Hardcover], April 11, 2017. Rosenthal: An American Sickness 2017
[30] Wikipedia, "Flexner Report 1910." Wikipedia Flexner Report
[31] Feld Stanley, "Repairing the Healthcare System," Feld: Repairing the healthcare system [31] Feld, ibid.
[32] Rosenthal Elizabeth "Paying till it hurts," The New York Times series on the costs of health care. Rosenthal: Costs of health care
[33] Rosenthal, Ibid. Rosenthal: An American Sickness 2017
[34] Emanuel Ezekiel J., Prescription for the Future, Public Affairs, New York, Reinventing American Healthcare, 2017. Emanuel: Future health care system 2017
[35] Fried, Ibid.
[36] Gross, Terry, "How Gross: US Health care big business 2017
[37] Huffman David, "Chronic Disease Today and Tomorrow," Huffman: Chronic diseases - today & tomorrow
[38] Jaffe, Ibid.
[39] Kliff, ibid.
[40] Mattke Soeren, Lisa Klautzer, Tewodaj Mengistu,Jeffrey Garnett, Jianhui Hu, Helen Wu, "Health and Well-Being in the Home: A Global Analysis of Needs,Expectations, and Priorities for Home Health Care Technology," Rand Health, 2010. Mattke: Rand-Home health care 2010
[41] Padula, Ibid.
[42] Shaw Michael D., "Chronic Disease: Some Interesting Theories And A New Book," Huffington Post, February 27, 2017. Shaw: Chronic disease theories 2017
[43] Weiss Martin, "The Great Medicare Rip-off of 2014," Weiss Investments. Weiss: Medical rip-off
[44] Shackelford Karen, "An emergency physician goes to the ER, and is shocked at the care she receives," MedPage, November 2, 2015. Shackelford: MD shocked at cost & service 2015
[45] Rosenthal, Rosenthal: Costs of health care
[46] Sorochan Walter, " Insurance Needs Big Numbers," Freegrab.net, September 25, 2014. Sorochan: How insurance works 2014
[47] Sorochan, Ibid.
[48] Brodwin Erin, "A coalition of the most advanced countries summed up what's wrong with America," Business Insider Science, June 23, 2017. Brodwin: Advanced countries view US Health care 2017
[49] Dept of Professional Employees, "The U.S. Health Care System: An International Perspective," Dept of Professional Employees: international perspective US health care system
[50] Pearl, ibid.
[51] Komlos John, KPBS Newshour, "Column: Here’s what’s wrong with the U.S.health care system," Politics, September 22, 2017. Komlos: KPBS What's wrong with US hea care sys 2017
[52] Kaiser Family Foundation, "Health Care Costs: A Primer, Report, May 01, 2012. Kaiser Report 2012
[53] Mattke Soeren, Lisa Klautzer, Tewodaj Mengistu,Jeffrey Garnett, Jianhui Hu, Helen Wu, "Health and Well-Being in the Home: A Global Analysis of Needs, Expectations, and Priorities for Home Health Care Technology," Rand Health, 2010. Mattke: Home health care 2010
[54] US health Agencies, OUTLINE OF US HEALTH AGENCIES. US Health Agencies
[55] Brodwin, Ibid. Brodwin: Advanced countries view US Health care 2017
[56] Komlos, Ibid.
[57] Yong, Ibid.
[58] Kaiser Family Foundation, Ibid.
[59] Marvasti Farshad Fani and Randall S. Stafford, "From Sick Care to Health Care — Reengineering," N Engl J Med, 2012; 367:889-891. Marvasti: re-engineering health care 2012
[60] Marvasti, Ibid.
[61] Horowitz, ibid.
[62] Marvasti, Ibid.
[63]Rosenthal, Ibid. Rosenthal: An American Sickness 2017
[64] Moynihan Shawn, "Health care: The Future is Now, BenefitsPro, April 2016. Moynihan: Health future is now 2016
[65] AMA staff writer, "What's at stake in nutrition education during med school," AMA wire, July 23, 2015. AMA: Nutrition status in medical schools 2015
[66] Adams Kelly M, Karen C. Lindell, Martin Kohlmeier and Steven H. Zeisel, "Status of nutrition in medical schools," NutritionFacts.org, 2011 [vodeo]. Adams: Nurtition education in medical schools 2011
[67] Marvasti, Ibid.
[68] Psaltopoulou, Ibid.
[69] Coulston Ann M., Cheryl L. Rock and Elaine R. Monsen, "Nutrition in the Prevention and Treatment of Disease," The American Journal of Clinical Nutrition, September 02, 2002; Hardcover book: The Prevention and treatment of Disease, [Book] Academic Press, London, 2001. Coulston: Disease prevention/treatment
[70] Christenson, Ibid.
[71] Christenson, Ibid.
[72] Lazonick William, Matt Hopkins, Ken Jacobson, Mustafa Erdem Sakinç and Öner Tulum, "US Pharma’s Financialized Business Model," Institute for New Economic Thinking, Working Paper No. 60, July 13, 2017. Lazonick: Pharma business model 2017
[73] Pearl. Ibid.
[74] Parramore Lynn, "Worse than big tobacco: How big pharma fuels the opioid epidemic," Institute for New Thinking, October 10, 2017. Parramore: Pharma fuels opioids 2017
[75] Hassner Sharav Vera, "Conflicts of interest," Alliance for Human Research Prediction [AHRP] Presentation before US Army Medical Deptartment, May 6, 2002. Hassner: Conflicts of interest 2002
[76] Angell Angell: Medical-drug corruption 2009[77] McGreal, Ibid.
[78] Cohen Joshua T & others, "Perspective - Does Preventive Care Save Money? Health Economics and the Presidential Candidates, N Engl J Med 2008. Cohen: Prevention & politics 20108
[79] Padula, Ibid.
[80] Consumer Report, "Hazardous health plans Coverage gaps can leave you in big trouble," May, 2009. Consumer Reports: Hazardous coverage 2003
[81] Cowan Dave, November 16, 2003. Cowan: 2 Suppresion Cowan: 2003
[82] Sorochan, Walter, "New medical Revolution," freegrab.net, April 14, 2012. Sorochan: New medical Revolution 2012
[83] Donohoe Gabriel, "Is Modern Medicine Founded on Error?" Natural News, December 07, 2007. Donohoe: New Medical Theory 2007
[84] Consumer Report Staff, "Hazardous health plans," Consumer Report, May 2009. Consumer Report: Health Plans 2009
[86] Steinreich Dale, "100 Years of US Medical Fascism," Mises Daily, April 16, 2010. Steinreich: !00 years of medicine 2010