By Walter Sorochan, PhD, MPH, MSc, BPE
Emeritus Professor San Diego State University
[ Posted May 13, 2009 ]
| This author was motivated to rebut an article, "What You Can
Expect from Socialized medicine," that appeared in an e-mail
advocating investment opportunities. The e-mail article focused on saving health care workers, insurance companies and pharmaceutical corporations in the business of making money and less focus on providing adequate and responsible health care. The article attempted to point out that national health care would displace many persons and entities and force them to find new ways of making money. Unfortunately, this attempt was also to discredit a national single-payer insurance carrier. The e-mail article focused on the miniscule issues that are irrelevant to what health care is all about. [ Traynham ] |
Health care reform in US
Socialized health care is a meaningless hypocritical term that has outlived its usefulness! The term can refer to any system of medical care that is publicly financed, government administered, or both. This narrower usage would apply to the British National Health Service hospital trusts and health systems that operate in other countries as diverse as Canada, Australia, Latin American countries, Finland, Spain, Israel and Cuba. The United States' Veterans Health Administration, and the medical departments of the U.S. Army, Navy, and Air Force would also fall under this narrow definition.
Canada's Medicare system, most of the UK's NHS general practitioner and dental services, which are all systems where health care is delivered by private business with partial or total government funding, fit this broader definition, as do the health care systems of most of Western Europe. In the United States, Medicare, Medicaid, and the U.S. military's TRICARE fall under this definition.
In conclusion, United States has many examples of already functioning public subsidized health care systems that can be labeled as socialized medicine. So labeling a single-payer health insurance carrier as socialized medicine has just lost its knock out punch as an argument!
 Lets face it, we are behind the rest of the world in providing
responsible health care! Some advocates complement the American medicine
as the best in the world but this is most disputable! It depends on what
one chooses as the basis for these arguments. But for now, United States
is the only country in the world that does not have national health
care!
Health care reform in US How do Americans feel about their health
care future:
Lets face it, we are behind the rest of the world in providing
responsible health care! Some advocates complement the American medicine
as the best in the world but this is most disputable! It depends on what
one chooses as the basis for these arguments. But for now, United States
is the only country in the world that does not have national health
care!
Health care reform in US How do Americans feel about their health
care future:
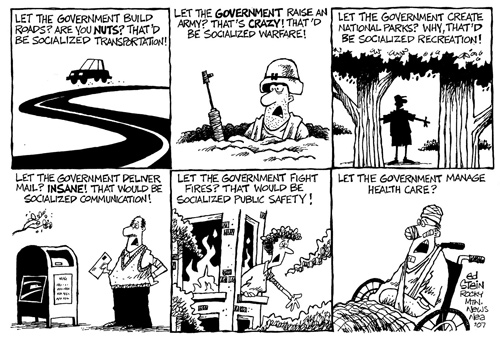
"But many Americans are ahead of the rhetoric. According to research reported in the Los Angeles Times on Feb. 25, few people are taken in by the boogeyman phrase. Robert Blendon, professor of health policy and political analysis at the Harvard School of Public Health, found that of the 67% of people who said they understood the meaning of "socialized medicine," 79% thought it was a good thing. He also found a political divide: 70% of Republicans thought socialized medicine would make the U.S. healthcare system worse; 70% of Democrats thought it would improve the system." Susan Brink Credit: Ed Stein / Rocky Mountain News, Socialized medicine and the presidential race, 3:49 PM, April 17, 2008
{kind=link}
The bottom line in switching from a "for profit messed up group of insurance carriers" is money! Money as controlled by vested political entities.
Yes money or how to pay for a system that is financially broke and dysfunctional. When a for-profit insurance carrier is not providing health care in a responsible manner, then it does not provide a service to the people! This is the reason to change to a single payer carrier system. To understand and appreciate the gist of these statements, one needs a history background on how the current medical system came into being and the big idea behind insurance. Another aspect of the switch to single-payer insurance system has to do with the ethics of whether anyone should be allowed to make money on sick and disabled persons! And thirdly, who has the responsibility to provide care for all citizens in any country and how to do this. Each of these issues must be addressed from an ethical, philosophical and realistic points of view.
Issue of Money: The current health care system of United states is financially broke and it is bankrupting United States. Money would probably be of lesser importance if all the people were covered by the current helter-skelter system. But there are over 50 million persons, about one-sixth of the total population, that are without adequate or no health insurance.
Health and economics are inter-related. The health of citizenry is directly related to the economy of a country. Sick workers cannot produce as much Gross National Product [ GNP ] as healthy workers can. In the failing economy of today, where banks, auto companies, airlines and big business are going broke and asking for bailouts and out-sourcing jobs and manufacturing to foreign countries to save money, we need healthy workers to compete with workers in other countries. One of the major reasons the auto companies are unable to compete with foreign markets is because providing health care to auto workers in United States wipes out profit. In an attempt to save money, American auto companies out source building many autos to Canada, where auto workers are automatically covered by the single-health insurance carrier. Canadian produced autos cost less because the health care coverage is much lower than in United States.
But the real advantage of a single-carrier system is economics. It is based on the fundamental concept of insurance: "The more persons covered the less the cost of premiums to all those in the insurance umbrella." A national single payer can cover millions more at much less cost than for profit insurance carriers can; hence the cost of health insurance becomes affordable for everyone. Numbers do make a difference! What is health insurance?
National health insurance in many countries allows competitive for-profit insurance carriers but subscribers find these to be much more expensive than the national health care option. These carriers will need to adopt and find other ways to make money. Likewise, medical workers will be retrained and recycled into useful and meaningful jobs. Pharmaceutical companies will also be forced to re-tool their research and development and how they provide medications.
Justification for government controlled medicine:
When should a government program supersede a private one? This
question can be resolved on a moral and ethical basis.
The
moral basis for national health
care is a very simple one. An analogy for this can be
found in parenting. A father as a parent is responsible for taking care
of his children. He provides the food and shelter for his children when
his children are too young to do so. And so it is with a national
government. A government acts in "loco parentis" or as a father of its
citizens.
The economic basis for a
government running a program can be illustrated with infrastructure
examples.
There are several good examples of private funded versus government
tax-funded projects to provide social, health and economic benefits to
people. An early attempt in United States and Europe to provide safe
drinking water to communities and cities occurred from 1800 to 1850.
Private enterprises were unable to provide safe drinking water. Public
distrust and alarm, and the deaths of many from water-borne diseases,
forced the local governments to intercede and do what private enterprise
could not. [ Colgrove, Ewbank, Flynn,
Harper, McKeown, Patel, Quinn, Szreter ]
The reader needs to be cognizant that health of the public was a primary
concern as increasing congestion in the urban environment heightened
pollution of local water sources that resulted in the spread of typhoid,
cholera and other water-borne diseases. Additionally, the provision of a
city-wide water supply was important to many businesses and industries.
Providing a safe water system became one of the most important ways that
a city could demonstrate its commitment to economic growth. Industry
needed healthy workers! This put pressure on local governments to
provide a healthy environment for workers.
The shift of most cities, especially large ones, to put ownership of
water systems as a public utility by the close of the 19th century was
also motivated in part by negative experiences with private water
suppliers. Private water companies “were notorious for choosing a
water source that would minimize the initial investment outlay, and for
ignoring the concomitant shortcomings in water quantity and quality.”
Lacking incentives to complete ostensibly unprofitable projects,
companies “preferred to lay their distributing pipes through the
wealthier sections of the city and to hold back from carrying water into
the poorer districts. Additionally, the public distrusted private
companies when drinking water they supplied was unsafe and the supply
unreliable. Private water companies were also more expensive than
most municipal suppliers – by as much as 40% by the close of the
century.
Government intervention:
Protecting the general public from communicable diseases
and providing a healthy work force to an expanding industrial economy:
The government has stepped in, on numerous occasions, to resolve
public benefit programs to ensure that services were provided without
discrimination and at fair prices to masses of people in all areas of
the country. Such government interventions became popular in resolving
many infrastructures. Industry demanded that their workers be assured of
staying healthy by having clean and safe drinking water. City
governments realized that this could only be done by creating a public
utility service; in other words, providing water as an infrastructure
for a city and its residents. Public taxes subsidized urban public water
and sewers, thus reducing mortality from waterborne diseases, improving
the health of workers and providing a healthy work force. These were
amenities that the private sector at that time was unable to do.
Public distrust of private companies during the early industrial
expansion days fomented a public outcry for government intervention.
Supplying water to cities is not the only example of government
intervention in subsidizing infrastructures. Railroads were another good
example where the government, during the 1820-1900 era of booming
industrial expansion, had to intervene in the private sector. The first
railroad in United States, the Baltimore and Ohio, began running in
1827. Railroads, financed by private enterprise, expanded rapidly to
transport freight and passengers. Fierce competition and political
fighting among railroad moguls resulted in disruptive public services
and railroad monopolies. [ Panariello ]
Supplying electricity to the city of New York and surrounding areas in
the 1920's likewise eventuated in public electric utilities. Building an
electrical grid to transmit electricity has become a history of
reoccurring blackouts and disputes. Our current electrical grid to supply
electricity to all sectors of the population and industry was built in
the early 1920's. Although it is outdated and needs to be replaced with
a "Smart Grid" current private utility corporations are reluctant to do
so; primarily because of the enormous expenses in doing do. This
presents a "who does it" dilemma for the government and utilities as the
current grid cannot support an ever-increasing demand for electricity.
Then there is the Eisenhower super-highway building project that only
the federal government could subsidize and build.
[ Belleranti, Gold, Panariello ] The
building of the first internet was an unknown and risky venture and was
initially subsidized by the federal government. These are ample examples
that illustrate the appropriateness of government to intervene when the
private sector cannot take the risk.
 Labeling national health care as socialized medicine is dispelled on
the basis of moral and economic grounds. There has to be a central
figure in overseeing the public good of a country. The private sector
does not do this when it is motivated by making money. Government has a
role in providing the spark for private entrepreneurs to participate in
providing services to the public. Numerous infrastructure examples,
mainly a safe water supply, are used to illustrate reasons why
government intervention may be necessary. Today as in previous
centuries, water must be seen to have economic value and not simply
stand as a social good. This concept of a safe water supply having
economic benefits needs to be transferred to thinking of national health
care as being essential to providing a competitive edge to our
industries and economy. What the private sector cannot do or
unwilling to spend money on is left to the government to put in place!
Government run programs have their flaws but related flaws are also
found in the private commercial sector as well. There are no saints,
only lesser evils!
Labeling national health care as socialized medicine is dispelled on
the basis of moral and economic grounds. There has to be a central
figure in overseeing the public good of a country. The private sector
does not do this when it is motivated by making money. Government has a
role in providing the spark for private entrepreneurs to participate in
providing services to the public. Numerous infrastructure examples,
mainly a safe water supply, are used to illustrate reasons why
government intervention may be necessary. Today as in previous
centuries, water must be seen to have economic value and not simply
stand as a social good. This concept of a safe water supply having
economic benefits needs to be transferred to thinking of national health
care as being essential to providing a competitive edge to our
industries and economy. What the private sector cannot do or
unwilling to spend money on is left to the government to put in place!
Government run programs have their flaws but related flaws are also
found in the private commercial sector as well. There are no saints,
only lesser evils!
A country is only as strong as its weakest link … the single citizen. It
is essential for a country to provide opportunities for the majority of
people and not just the few. The welfare of the masses is more important
than that of just a few.
References:
Belleranti Guy, "The 1950’s Birth of the Interstate Highway System,"
Rewind the Fifties.
birth interstate hyw
Brink Susan & credit: Ed Stein, "Socialized medicine and the
presidential race," Rocky Mountain News, April 17, 2008.
Colgrove James, "The McKeown Thesis: A Historical Controversy and Its
Enduring Influence," Am J Public Health. 2002 May; 92(5): 725–729
"The medical profession underwent a profound crisis of confidence in the 1970s, as advanced nations of the world, especially the United States and Great Britain, began to question large expenditures on sophisticated medical techniques that seemed to produce diminishing returns in quality of life. In contrast to the optimism and faith in medicine that had characterized the 1950s, the prevailing attitude toward the profession became one of cynicism, mistrust, and therapeutic nihilism."Ewbank DC, Preston SH. Personal health behaviour and the decline in infant and child mortality in the United States, 1900–1930. In: What We Know About the Health Transition: The Cultural, Social, Behavioural Determinants of Health—Caldwell J, Findley S, Caldwell P, et al, eds. (1990) Canberra: Australia National University Press. 116–49.
Flynn Sean & Bourdouris Kathryn,"DEMOCRATISING THE REGULATION AND GOVERNANCE OF WATER IN THE US," RECLAIMING PUBLIC WATER: ACHIEVEMENTS, STRUGGLES AND VISIONS FROM AROUND THE WORLD, ©January 2005.
_______, "Health care reform in the United States," Reform USA
Harper, Sam, "Did clean water reduce black–white mortality inequalities in the United States? Water, Race, And Diseases," International Journal of Epidemiology.
Gold Jenny, "A Modern Electric Grid: The New Highway System?" NPR. April 27, 2009. New Grid system
"In 1956, after several appeals from the president, Congress enacted the Federal-Aid Highway Act, creating an interstate system that now consists of nearly 47,000 miles of highway and took 50 years to build.McKeown T., The Modern Rise of Population, Academic Press, New York, 1976.
"The interstate highway system is absolutely part of the country. It seems so natural and logical to us. But in the 1950s, it was a radical thought," says Susan Eisenhower, president of the Eisenhower Group and granddaughter of President Eisenhower.
Morrison Bob, "High Speed Trolleys - 1: A Practical Solution for Today's Traffic Problems,"
Panariello Halina, "Social Studies: World History: Railroads of Asia, America, and Britain," Homework Help, May 07, 2009. railroad history
Patel Kant & Rushefsky Mark E., The politics of public health in the United States, M.E.sharpe, December, 2005.
Porter Dorthy, Health, Civilization and the State: A History of Public Health from Ancient to Modern Times (Paperback)
"two key factors in the limited approach to public health reform in the United States: the public's distrust of the medical community and opposition by business leaders to expensive changes."Quinn Timothy, Calif. Water Supply Crisis Affecting Economy,Water & Wastwater News, April 21, 2008. [ACWA Executive Director Timothy Quinn ]
"For the first time in a long time, California is losing income and jobs because our water supply system is in crisis," Water must be seen to have economic value and not simply stand as a social good.Szreter S., "The importance of social intervention in Britain's mortality decline c. 1850-1914: a reinterpretation of the role of public health," Soc Hist Med. 1988;1:1–38.
Decisions on new housing and retail developments in Riverside County are on hold because the necessary water supplies cannot be guaranteed. One of the delayed projects, a major distribution center, was expected to generate 1,000 jobs.
Growers in northern San Diego County are stumping citrus and avocado trees due to water shortages."
In Szreter's new interpretation of the data, public health measures such as clean water and milk supplies assumed greater importance, while changing social conditions, to which McKeown had attributed beneficial effects such as improvements in nutrition, were in fact a detrimental influence, resulting in, for example, overcrowded and poorly constructed housing resulting from rapid urbanization.Troesken W. Water, Race, and Disease, MIT Press, Cambridge, MA. 2004.
Traynham Lindy Brady, "What You Can Expect from Socialized medicine," Whiskey & Gunpowder, May 5, 2009.
What are predictable results of government ramming socialized medicine down our throats? We can’t stop the programs, so how can we make money from the ineluctable outcome? A few ideas spring to mind immediately:
1.
Has it dawned on anyone in Washington that Socialized medicine just might have some slight effect on insurance companies? It might be time for us to consider shorting a few viciously...or is that still illegal?!The health insurance rack...ah, business...is one of the largest in America. The law as proposed will make it illegal to have private insurance to supplement the government’s "single payer" plan. A major portion of the GDP will be destroyed in that area alone. What will happen to those who currently underwrite supplements to Medicare?
No one can prognosticate how many irrational requirements, forbidden activities, and finable offenses will come out of the final legislation, but we can certainly conclude that this shake up and shake down is going to be off the Richter Scale in terms of lost jobs and destroyed capital. When the government is the HMO there is no place for a private HMO.
2.
The proposed law also makes it illegal for doctors to provide services outside of the system and it will determine what doctors and hospitals are paid. This is certain to lead to staff shortages, probably more quickly than we are anticipating.A.
How many older doctors will retire rather than submit? Why should they work just as hard for a great deal less money? Why should they tolerate having their medical judgment overridden by a bunch of penny-pinching bureaucrats? "First, do no harm" also prohibits doing nothing when treatment is indicated clearly.B.
How many physicians are already considering retiring from the practice of medicine because of the proposed ukases which would require them, under penalty of law, to perform abortions on demand?C.
Any young student with the brains to make it through medical school will tend to decide quickly that it would be far more sensible, faster, and lucrative to become a dentist or a veterinarian. Any good vet makes at least $100K, but socialized doctors don’t. This isn’t guesswork; it is the experience in Canada and England. A quick perusal of the literature reveals also that it is best not to become ill after June and that a dog can get an MRI the same week but people wait months, if they get them at all.3.
What effect will this have on the cost of medical and nursing schools? Silly question; tuition will go up because it costs the same amount to offer instruction and classrooms whether they are full or half full. We can prognosticate that less qualified applicants will be admitted because fewer will apply. Corners will be cut wherever possible. Fewer courses will be offered. Why train in procedures likely to be forbidden? Standards will be lowered. It may even become a great deal easier to pass the exams to be able to write "M.D." after one’s name.4.
What is to be done with the clerks in all doctors’ offices who do nothing except handle insurance paperwork — and keep their doctors up to date on how to write up bills and lab requests to obtain the greatest return from insurance companies? Some of them may find jobs in the new bureaucracy, but one putative benefit of socialized medicine is that less paperwork will be needed to provide better records. Good insurance clerks are paid well, and deservedly so, for theirs is specialized work. We can suppose that those who train typists to transpose doctor’ s recorded notes may find less business (knocking out their schools and a good at home source of income for quite a few), because a pretty good guess is that over-scheduled, under-paid doctors aren’t going to generate the sort of records we are accustomed to now.5.
The AMA and insurance companies have enormous lobbies, which makes one wonder why there isn’t any outcry from those areas. That is really a very interesting point upon which to speculate. What does the AMA expect to get out of this that is worth the price of tolerating bureaucrats to set fees and determine procedures? Do they think that going along will prevent even more Draconian cuts and restrictions, or can someone in the Bar today come up with a better answer to "Cui bono?"6.
Pharmaceutical companies spend lots of money in Washington; could it be that they do not expect the prices of their products to be cut as proponents of socialized medicine insist is one way costs will be controlled? Perhaps a lessening of the restrictions that make developing a new drug cost billions has been tendered? Again, what’s in it for Merck and Roche and Lilly not to scream their heads off? A good prediction is that only generics will be allowed to be prescribed, which is bad news for those of us for whom Synthroid is not an adequate substitute for Armour Thyroid, and a very nasty lump for Armour, which gets $90 from me, alone, every time I fill my prescription, instead of three or four bucks. What is the point of developing proprietary drugs if the cost cannot be recou ped many times over?7.
We old-timers are being told we will simply have to learn to live with our aches and pains and that services will be cut for us in order to care for the younger population better. Doesn’t it make you feel all warm and fuzzy to know that you may not get a life-saving procedure because it "costs too much at your time of life and the money will be better spent on millions of lawbreakers granted amnesty and citizenship, instead?" Already there are services to help us find superior medical and dental care at deeply reduced prices in India, for example. However, if/when "Cap and Trade" is pushed through, what is that going to do to the airline industry? We may well end up with no viable way to obtain adequate health care at any price short of suborning our private ph ysicians. I joked with mine when I saw him for routine blood work a couple of months ago that between the coming depression and socialized medicine we might end up skulking to meet in an alley at midnight, me with a chicken in my hand. My brilliant young physician, with enormous student loans, looked grim, and said, "I’ll take it!" Back in The Great Depression a chicken was considered a good fee, by the way.8.
Where will peripheral specialties come into all of this? Lasik surgery, for example. Will such surgeons be exempted, or will they be driven out of business because glasses were good enough for Benjamin Franklin?"Is there a lawyer in the house?" It will, one can only suppose, be forbidden for medical personnel to assist in times of crisis, accident, or disaster since the law as drafted forbids practicing outside of the system. Few do anyway these days because of the danger of lawsuits.
If anyone here will admit to being an attorney, please take a shot at explaining the Constitutional justification for government controlled medicine, since it obviously isn’t going "to promote the general welfare." While you’re at it, explain how anyone can justify making it a crime for a duly trained and licensed doctor to treat patients who seek his care.
For preliminary actions...just off hand, I would not invest in a chain of dialysis clinics or expect MRI apparatus to sell as well. We should probably be leery of many pharmaceutical companies. On an individual level, it might even be a good idea to go get heart by-pass surgery now if you expect to need it in the next few years, although there are better choices.
So...I’ll raise my glass of Lambrusco (full of healthful substances and a modest jolt of alcohol), and look forward to hearing your views on how to profit from what is coming our way.
Regards,
Linda Brady Traynham